Whitney Tilson’s email to investors discussing the severity of coronavirus (CV) and the number of confirmed CV cases.
I was initially much too dismissive of how severe the CV would be and the societal reaction to it, so (perhaps partly as penance!) I’m going to make a big effort to “cloud-source” the best information, articles, and opinions out there – and add a little of my own thinking and commentary. In doing so, I hope to both educate – and be educated!

Q4 2019 hedge fund letters, conferences and more
I’m catching up on a weekend’s worth of reading and emails so this email is very long. Future emails will not be – many, in fact, will simply be links to an article of interest, with a quick comment, nothing more…
Rise In The Number Of Confirmed CV Cases
1) My view right now – with much humility, recognizing the very wide range of possible outcomes – is that things are going to be very bad for at least the next 2-3 weeks, both economically, as the world largely shuts down (as it should!), and emotionally, as the number of confirmed CV cases (due to testing identifying both newly infected people as well as those infected earlier) and deaths rise sharply (accompanied by non-stop frightening headlines).
This is what happened in China.
But then I think the rest of the world, like China, will get a handle on this scourge, the number of new cases and deaths will start to fall (even without the possible benefit of warmer weather, which would be a huge bonus), and, over many months, we will recover, both economically and emotionally.
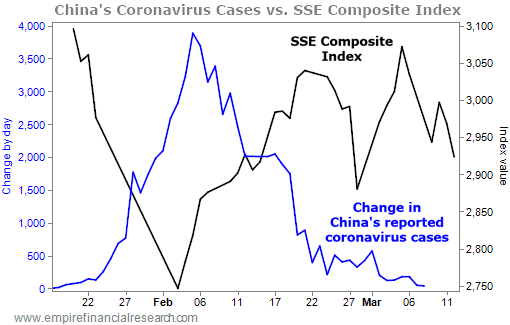
Anticipating this, stock markets could recover (at least partially) quite quickly (again, like China), which is why I think it’s the best time to be an investor since 2008-2009. Here is a chart I included in my email on Friday to the 35,000 people on my daily investing email list, showing that the Shanghai stock exchange rebounded sharply at almost exactly the same time that the number of new CV cases began to decline:
You can Friday’s email in its entirety here: What a day!; Why I'm trembling with greed; Two critical developments; When I think stocks are likely to bottom; When do you think they will?; Are you an investor or a speculator?
And you can sign up for my investing email list here.
2) If you’re following the markets, I’d be grateful if you’d take a few seconds to fill out this survey I included in Friday’s investing email:
In yesterday's e-mail, when the S&P 500 was at 2,500, I wrote: "I would guess that... we're within 5% to 10% of the ultimate bottom."
I'd be very curious to hear your best guess about where the index will bottom, as well as when it will recover its losses and hit a new high (meaning it rises 36.4% from yesterday's close). I believe in the "wisdom of crowds" (to quote the title of the excellent book by James Surowiecki), so I would be grateful if you'd take 10 seconds to fill out this two-question survey I posted here. I will share the results next week.
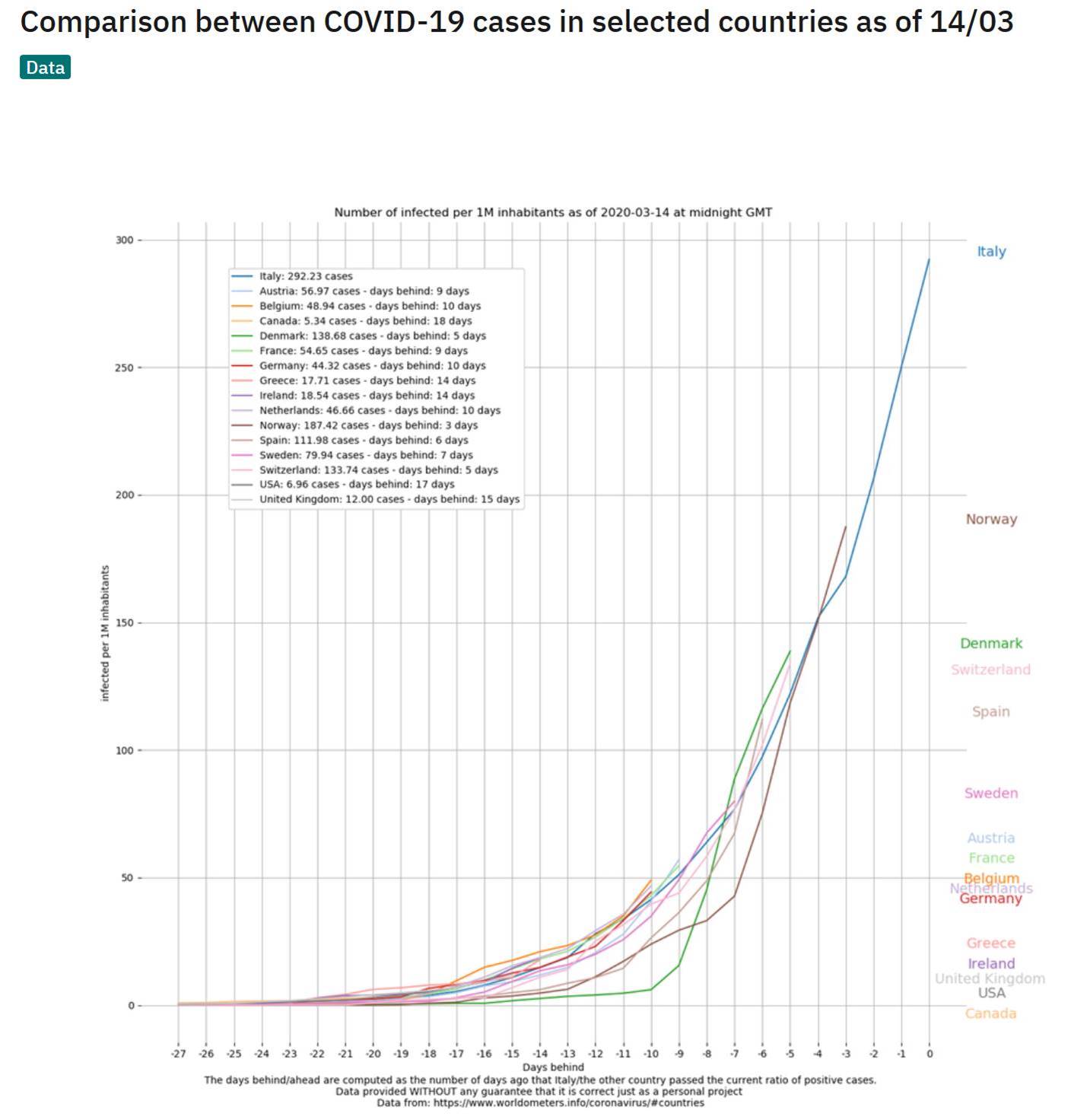
3) This chart (posted yesterday) sums up why governments around the world are taking drastic actions – it tracks number of confirmed CV cases per million inhabitants, on a lag of days behind Italy. Virtually all are following the same trend line. The good news for the U.S. is that it’s the furthest behind – 17 days – so hopefully the strong actions we’re now taking will mean we don’t follow Italy…
Humantiy Will Survive
4) This Nobel laureate and Stanford professor correctly predicted what happened in China, in response to the country’s drastic actions. Let’s hope he’s right that the rest of the world will follow the same trajectory! Corona Is Slowing Down, Humanity Will Survive, Says Biophysicist Michael Levitt. Excerpt:
“The rate of infection of the virus in the Hubei province increased by 30% each day—that is a scary statistic. I am not an influenza expert but I can analyze numbers and that is exponential growth.” At this rate, the entire world should have been infected within 90 days, he said.
Italy In A Lockdown
5) Italy is in complete lockdown – friends are sending me videos of deserted streets, even in the south, which hasn’t been hit (yet) – which should lead to a peak in new CV infections soon, but right now the numbers are still getting much worse: in the past 24 hours, 3,590 new cases and 368 deaths. Here’s a powerful article by an Italian journalist: A coronavirus cautionary tale from Italy: Don’t do what we did. Excerpt:
So here’s my warning for the United States: It didn’t have to come to this.
We of course couldn’t stop the emergence of a previously unknown and deadly virus. But we could have mitigated the situation we are now in, in which people who could have been saved are dying. I, and too many others, could have taken a simple yet morally loaded action: We could have stayed home.
6) In contrast to the rest of the world, Britain’s Prime Minister is rolling the dice is a big way. I think odds are high that he’s making the wrong decision, but there’s a small chance he’ll be proven right, which would have important implications for how the world handles future pandemics… As Europe Shuts Down, Britain Takes a Different, and Contentious, Approach. Excerpt:
“There’s no other country in the world managing the epidemic in the same way,” Francois Balloux, an infectious disease epidemiologist at University College London, said of Britain’s approach. But, he said, “It’s not an insane decision. And it might actually pay off.”
7) This post has more than 28 million views: Coronavirus: Why You Must Act Now. Excerpt:
You might have fears today: What if I overreact? Will people laugh at me? Will they be angry at me? Will I look stupid? Won’t it be better to wait for others to take steps first? Will I hurt the economy too much?
But in 2–4 weeks, when the entire world is in lockdown, when the few precious days of social distancing you will have enabled will have saved lives, people won’t criticize you anymore: They will thank you for making the right decision.
Ok, let’s do this.
CV cases Simulator
8) Here’s a “coronavirus simulator” in the Washington Post that runs random simulations for a free-for-all, an attempted quarantine, moderate social distancing and extensive social distancing: Why outbreaks like coronavirus spread exponentially, and how to “flatten the curve”. Here is a graphic of the results:

9) My friend Anton Wahlman with two arguments why the CV may not spread as rapidly here: America’s Cars And Low Population Density May Be Key To The Low Virus Impact. Excerpt:
- If it turns out that the latest virus scare impacts the U.S. less than most other countries, we will need an explanation.
- In this article, I offer a theory that consists of two factors: Population density and individual car ownership.
- Basically, in the U.S. we have a much lower population density than most other relevant countries, and we are far more prone to drive our own car.
- In those other countries, more people are cramped into high-rises, and they ride the bus or take the train/subway to/from work.
- It only stands to reason that you are far more protected against bugs if you live in a house on a large lot and drive your own vehicle to and from work.
10) Here are what two of my friends report from Hong Kong, Singapore, and Shanghai:
Good news I heard today directly from friends in Hong Kong & Singapore: life is getting back to normal there. In Singapore, the malls and supermarkets are full of people again. In HK life is 70-80% back to normal and people have started regular working hours again.
Not so good news: Europe is probably three weeks behind Asia with less severe restrictions, less experience in tracking infected people, and less testing (Asia was better prepared because of the SARS experience) – and the US is probably three weeks behind Europe….
So six more weeks of bad news and increasing infections before we have reached the global peak (??). Unknowable of course…..but a reasonable guess (?). Question how markets will react in the interim….unknowable too….but likely to remain very volatile ….have we seen the max. drawdown already when peak infections are at least 2-3 weeks away???
And this is what a longtime friend from Shanghai emailed me a week and a half ago:
Generally things are getting back to normal in Shanghai, though it is definitely a new normal, with ubiquitous screening monitoring. Retail is still struggling, but subway ridership and vehicle traffic are starting to get back to normal levels, and various manufacturing firms that we follow are steadily increasing production capacity (now ranging from 40%-60%), despite staffing and supply chain issues. In short, everything is gradually starting to come back, though there's lots of concern regarding folks returning to Shanghai from international destinations...
Our teenage son's middle school has been operating for the last few weeks with online/remote learning. This past Monday, Shanghai commenced the operations of twelve television stations, one for each grade 1-12, with daily lessons from Shanghai's prescribed curriculum. The city hasn't yet set the date for school reopenings, but it certainly won't be earlier than April.
11) Some of my friends are skeptical that the U.S. or Europe will be able to replicate the success China and South Korea have had containing the CV. One wrote:
The more I read about China’s actual response, the more I am convinced that no country can even come close to what they did - especially in the West. According to this article, their response was completely beyond what the WHO recommends. It appears that the only reason it worked so well is because of the complete control they have on their people. This may seem obvious, but it involves much more than just enforcing lockdowns. Check out this article in the WSJ: How China Slowed Coronavirus: Lockdowns, Surveillance, Enforcers. Excerpt:
Authorities sealed off Wuhan, a city of 11 million, on Jan. 23. At least a dozen more lockdowns followed. The party dispatched armies of low-level enforcers to guard the gates of residential compounds and restrict the movements of people living inside.
Another added:
No way we will quash this like they did. Another reason why is we have too many epicenters. CA Washington/ New York / MA / NJ. New Hampshire has only tested 56 patients and 50+ are positive. Who knows how many more are out there.
Interesting how they all are north-ish.
We can’t get tests we can’t get masks. This is a joke.
A third (a Chinese American) added:
We absolutely cannot replicate the Chinese and South Korean response. I've heard from people on the ground in these countries that if you go anywhere (take a bus, go to the grocery store, etc.), your temperature is taken and if you have a fever you are not allowed into the establishment. These countries are also much more technologically connected than we are. The smartphone is used in every person's life even the elderly. For example my grandparents, who are in their 90s, are very proficient cell phone users who use electronic payments, ride sharing, etc. They have COVID alerts that tell people whether there has been an infected person who has visited a grocery store and at what time. If you were in the area around the same time, you are notified and are tested as well.
12) Expect to see more headlines like this: Goldman Takes Out The Chainsaw: Cuts US Q2 GDP To -5%; Says Recession Has Begun. Excerpt:
As a result, the bank is now expecting Q2 GDP to crater -5%, down from its prior forecast of 0%, and the biggest quarterly GDP contraction since the peak of the financial crisis when GDP cratered by 8.4%.
13) Credit markets are seizing up, though I have no doubt that governments will quickly intervene: Key Source of Corporate Cash Seizing Up Amid Credit Market Rout. Excerpt:
................
Money Fund Risks
“The Fed needs to come in and serve as the buyer,” Cabana, Bank of America’s head of rates strategy and a former officer in the New York Fed’s markets group, said in an interview Sunday. “It’s prudent for everyone to try and raise liquidity, and the Fed needs to facilitate this.”
14) Stories like this don’t help the markets… The Washington Post: Infighting, missteps and a son-in-law hungry for results: Inside the Trump administration’s troubled coronavirus response. Excerpt:
This is exactly the shit-show that has characterized the entire administration of the Malignant Toddler and his ass-kissing toadies - but in this case, their bumbling incompetence and infighting will lead to a lot of people dying needlessly... Excerpt:
Kushner entered into a crisis management process that, despite the triumphant and self-congratulatory tone of public briefings, was as haphazard and helter-skelter as the chaotic early days of Trump’s presidency — turning into something of a family-and-friends pandemic response operation
15) Here’s an article about the 1957 Asian flu pandemic: Say Your Prayers and Take Your Chances. Excerpt:
,...........
Today, I look back and wonder if an oblivious America faced the 1957 plague with a kind of clueless folly. Why weren’t we more active in fighting this contagion? Could stricter quarantine procedures have reduced the rate of infection and lowered the death toll? In short, why weren’t we more afraid?
It’s hard to answer that question without explaining what it was like to grow up in an age of infectious illness.
The problem with these comparisons is that no prior pandemic (unless you got back to 1918) appears to have the same combination as the coronavirus of being both highly contagious and highly (but, ironically, not too highly) fatal…
16) I just signed up to receive email updates from the John Hopkins Center for Health Security site.
17) Some wise thoughts from a friend of a friend:
I am in a unique position to be providing an update on coronavirus because I have been helping to lead our work on understanding the market impact of the virus and I am also in self-quarantine because I was exposed to the virus at the Cowen healthcare conference in Boston last week. With all of the media coverage and a wide variety of “experts” making comments, plus the fact that available data is limited and changes each day, it is difficult to reach an objective view on the risk of covid-19.
Based on the work we have done including lots of expert discussions, modeling of the disease, and review of the emerging clinical literature and case reports, I can share with you our emerging view. Covid-19 is something to be taken seriously and some behavior modifications are important, but it is not worthy of panic and needs to be discussed in a fact based, objective way for people to appropriately manage both personal and professional risk.
Covid-19 is a coronavirus that is believed to have passed from animals to humans and is similar in some ways to SARS and MERS, two prior coronaviruses that infected humans. For both SARS (2002) and MERS (2012) the mortality rate was very high which led to low transmission rates. Covid-19 was first confirmed in China in December and has now been confirmed in 127k patients globally and implicated in 4,700 deaths.
One important thing to note is that the death count is likely very accurate as those patients are nearly always counted while the overall infection rate is likely very significantly understated because it is based on confirmed tests and the availability of testing has been highly limited in virtually all countries. So while you will see the death rate quoted as 2-4% using those numbers, the actual death rate is highly likely to be much lower. Two good examples are the infection and death rate on the Royal Princess Cruise Ship where everyone was tested – 3700 passengers, 696 confirmed cases, and 7 deaths, so 19% of passengers infected and a 1% death rate.
Also of the 696 cases, only half had symptoms so you can see that in a very close environment with substantial testing, the actual rates of infection, symptoms and death are well below the numbers typically quoted in the media. Other country experiences that are informative of what to expect are Singapore, South Korea and Japan where testing rates were high, infections ramped and then waned quickly and mortality rates among confirmed patients were in the range of 1%.
One brief side point on death rates – covid-19 has been found to cause death in most cases from your immune system over-reacting and attacking itself. This creates a “cytokine release storm” that typically ends up with lung failure. This tends to be more of a risk in older patients and in those with underlying conditions that put them at risk like smoking or hypertension. One very interesting observation to date is that children do get infected but do not seem to show any significant symptoms – the primary hypothesis for this is that the young immune system is more adaptable because it is still learning what pathogens to fight off and typically does not attack itself.
It is believed that children can spread the infection but that is not confirmed. Two other points, symptoms appear on average at 5 days and if you progress to severe infection, death typically occurs around 17 days post infection. The most common symptoms are flu like – cough, fever, diarrhea, fatigue.
Based on the work we have done, we believe covid-19 spreads primarily via “super spreaders” – that is a single individual who infects a large number of others who then typically will not go on to keep infecting more people. This is consistent with what was observed with both SARS and MERS where the spread was primarily due to single individuals rather than communities passing the infection around. What we believe happens is that someone who is infected grows very ill, likely due to age or lifestyle and then while they have a very high viral load, they pass the virus on to others.
While the media continues to suggest the virus passes through the lungs, the best available clinical literature suggests infection occurs most commonly through the passage of respiratory droplets from an infected person to the mucus membrane of an uninfected person – imagine a very sick person coughing on some forks in a salad bar basket and then others using those forks to eat, for example. That helps explain why it appears there are pockets of outbreak – that is common with super spreaders. Also, the viral genome has been studied extensively and it has been mutating – and contrary to the movies, viruses tend to mutate toward lower severity in order to increase their ability to spread.
That could partially explain why mortality rates are more modest in most countries now than the rates in China, Italy and Iran. But the other explanation for lower mortality is awareness is leading to better, earlier care.
As testing ramps up, we are likely to see a significant increase in confirmed infections but we are also very likely to see a decrease in the death rate. As mortality rate falls below 1% and continues to skew to the old and frail, we think calm will return. One last point – there is significant work being done on treatments and vaccines. They will not impact the infection in the near term but should the infection stick around and become a seasonal pathogen, we are likely to have vaccines and treatments ready and possibly as soon as a year from now.
So the chances of getting infected remain low, the vast majority of infections continue to resolve without significant complication and steps to reduce spread may or may not actually help depending on how much infection is already circling. What is most important is to practice standard good hygiene and seek medical attention if you start showing symptoms in an effort to avoid becoming a super spreader.
18) Here are notes taken by Scott Cook, the founder of Intuit (Quicken, TurboTax) from a discussion last Tuesday on COVID-19 with the top researchers in infectious disease at the University of California, San Francisco (UCSF is either the #1 or #2 hospital in California depending on which survey you read; it is the 4th largest medical research center in the US, based on research grants).
University of California, San Francisco BioHub Panel on CV cases
March 10, 2020
- Panelists
- Joe DeRisi: UCSF’s top infectious disease researcher. Co-president of ChanZuckerberg BioHub (a JV involving UCSF / Berkeley / Stanford). Co-inventor of the chip used in SARS epidemic.
- Emily Crawford: COVID task force director. Focused on diagnostics
- Cristina Tato: Rapid Response Director. Immunologist.
- Patrick Ayescue: Leading outbreak response and surveillance. Epidemiologist.
- Chaz Langelier: UCSF Infectious Disease doc
What’s below are essentially direct quotes from the panelists. I bracketed the few things that are not quotes.
- Top takeaways
- At this point, we are past containment. Containment is basically futile. Our containment efforts won’t reduce the number who get infected in the US.
- Now we’re just trying to slow the spread, to help healthcare providers deal with the demand peak. In other words, the goal of containment is to "flatten the curve", to lower the peak of the surge of demand that will hit healthcare providers. And to buy time, in hopes a drug can be developed.
- How many in the community already have the virus? No one knows.
- We are moving from containment to care.
- We in the US are currently where at where Italy was a week ago. We see nothing to say we will be substantially different.
- 40-70% of the US population will be infected over the next 12-18 months. After that level you can start to get herd immunity. Unlike flu this is entirely novel to humans, so there is no latent immunity in the global population.
- [We used their numbers to work out a guesstimate of deaths— indicating about 1.5 million Americans may die. The panelists did not disagree with our estimate. This compares to seasonal flu’s average of 50K Americans per year. Assume 50% of US population, that’s 160M people infected. With 1% mortality rate that's 1.6M Americans die over the next 12-18 months.]
- The fatality rate is in the range of 10X flu.
- This assumes no drug is found effective and made available.
- The death rate varies hugely by age. Over age 80 the mortality rate could be 10-15%. [See chart by age Signe found online, attached at bottom.]
- Don’t know whether COVID-19 is seasonal but if is and subsides over the summer, it is likely to roar back in fall as the 1918 flu did
- I can only tell you two things definitively. Definitively it’s going to get worse before it gets better. And we'll be dealing with this for the next year at least. Our lives are going to look different for the next year.
- What should we do now? What are you doing for your family?
- Appears one can be infectious before being symptomatic. We don’t know how infectious before symptomatic, but know that highest level of virus prevalence coincides with symptoms. We currently think folks are infectious 2 days before through 14 days after onset of symptoms (T-2 to T+14 onset).
- How long does the virus last?
- On surfaces, best guess is 4-20 hours depending on surface type (maybe a few days) but still no consensus on this
- The virus is very susceptible to common anti-bacterial cleaning agents: bleach, hydrogen peroxide, alcohol-based.
- Avoid concerts, movies, crowded places.
- We have cancelled business travel.
- Do the basic hygiene, eg hand washing and avoiding touching face.
- Stockpile your critical prescription medications. Many pharma supply chains run through China. Pharma companies usually hold 2-3 months of raw materials, so may run out given the disruption in China’s manufacturing.
- Pneumonia shot might be helpful. Not preventative of COVID-19, but reduces your chance of being weakened, which makes COVID-19 more dangerous.
- Get a flu shot next fall. Not preventative of COVID-19, but reduces your chance of being weakened, which makes COVID-19 more dangerous.
- We would say “Anyone over 60 stay at home unless it’s critical”. CDC toyed with idea of saying anyone over 60 not travel on commercial airlines.
- We at UCSF are moving our “at-risk” parents back from nursing homes, etc. to their own homes. Then are not letting them out of the house. The other members of the family are washing hands the moment they come in.
- Three routes of infection
- Hand to mouth / face
- Aerosol transmission
- Fecal oral route
- What if someone is sick?
- If someone gets sick, have them stay home and socially isolate. There is very little you can do at a hospital that you couldn’t do at home. Most cases are mild. But if they are old or have lung or cardio-vascular problems, read on.
- If someone gets quite sick who is old (70+) or with lung or cardio-vascular problems, take them to the ER.
- There is no accepted treatment for COVID-19. The hospital will give supportive care (eg IV fluids, oxygen) to help you stay alive while your body fights the disease. ie to prevent sepsis.
- If someone gets sick who is high risk (eg is both old and has lung/cardio-vascular problems), you can try to get them enrolled for “compassionate use" of Remdesivir, a drug that is in clinical trial at San Francisco General and UCSF, and in China. Need to find a doc there in order to ask to enroll. Remdesivir is an anti-viral from Gilead that showed effectiveness against MERS in primates and is being tried against COVID-19. If the trials succeed it might be available for next winter as production scales up far faster for drugs than for vaccines. [More I found online.]
- Why is the fatality rate much higher for older adults?
- Your immune system declines past age 50
- Fatality rate tracks closely with “co-morbidity”, ie the presence of other conditions that compromise the patient’s hearth, especially respiratory or cardio-vascular illness. These conditions are higher in older adults.
- Risk of pneumonia is higher in older adults.
- What about testing to know if someone has COVID-19?
- Bottom line, there is not enough testing capacity to be broadly useful. Here’s why.
- Currently, there is no way to determine what a person has other than a PCR test. No other test can yet distinguish "COVID-19 from flu or from the other dozen respiratory bugs that are circulating”.
- A Polymerase Chain Reaction (PCR) test can detect COVID-19’s RNA. However they still don’t have confidence in the test’s specificity, ie they don’t know the rate of false negatives.
- The PCR test requires kits with reagents and requires clinical labs to process the kits.
- While the kits are becoming available, the lab capacity is not growing.
- The leading clinical lab firms, Quest and Labcore have capacity to process 1000 kits per day. For the nation.
- Expanding processing capacity takes “time, space, and equipment.” And certification. ie it won’t happen soon.
- UCSF and UCBerkeley have donated their research labs to process kits. But each has capacity to process only 20-40 kits per day. And are not clinically certified.
- Novel test methods are on the horizon, but not here now and won’t be at any scale to be useful for the present danger.
- How well is society preparing for the impact?
- Local hospitals are adding capacity as we speak. UCSF’s Parnassus campus has erected “triage tents” in a parking lot. They have converted a ward to “negative pressure” which is needed to contain the virus. They are considering re-opening the shuttered Mt Zion facility.
- If COVID-19 affected children then we would be seeing mass departures of families from cities. But thankfully now we know that kids are not affected.
- School closures are one the biggest societal impacts. We need to be thoughtful before we close schools, especially elementary schools because of the knock-on effects. If elementary kids are not in school then some hospital staff can’t come to work, which decreases hospital capacity at a time of surging demand for hospital services.
- Public Health systems are prepared to deal with short-term outbreaks that last for weeks, like an outbreak of meningitis. They do not have the capacity to sustain for outbreaks that last for months. Other solutions will have to be found.
- What will we do to handle behavior changes that can last for months?
- Many employees will need to make accommodations for elderly parents and those with underlying conditions and immune-suppressed.
- Kids home due to school closures
- [Dr. DeRisi had to leave the meeting for a call with the governor’s office. When he returned we asked what the call covered.] The epidemiological models the state is using to track and trigger action. The state is planning at what point they will take certain actions. ie what will trigger an order to cease any gatherings of over 1000 people.
- Where do you find reliable news?
- The John Hopkins Center for Health Security site. Which posts daily updates. The site says you can sign up to receive a daily newsletter on COVID-19 by email. [I tried and the page times out due to high demand. After three more tries I was successful in registering for the newsletter.]
- The New York Times is good on scientific accuracy.
- Observations on China
- Unlike during SARS, China’s scientists are publishing openly and accurately on COVID-19.
- While China’s early reports on incidence were clearly low, that seems to trace to their data management systems being overwhelmed, not to any bad intent.
- Wuhan has 4.3 beds per thousand while US has 2.8 beds per thousand. Wuhan built 2 additional hospitals in 2 weeks. Even so, most patients were sent to gymnasiums to sleep on cots.
- Early on no one had info on COVID-19. So China reacted in a way unique modern history, except in wartime.
- Every few years there seems another: SARS, Ebola, MERS, H1N1, COVID-19. Growing strains of antibiotic resistant bacteria. Are we in the twilight of a century of medicine’s great triumph over infectious disease?
- "We’ve been in a back and forth battle against viruses for a million years."
- But it would sure help if every country would shut down their wet markets.
- As with many things, the worst impact of COVID-19 will likely be in the countries with the least resources, eg Africa. See article on Wired magazine on sequencing of virus from Cambodia.
19) A funny and heartfelt message from Trevor Noah, announcing that The Daily Show was closing for the next week and telling his audience to stay home: A Message from Trevor: Stay Home. Excerpt:
And another thing. Stop hoarding everything, guys. You don’t have to buy all the toilet paper, okay? Like, I don’t know what kind of sh*ts you’re having, but calm down. People need toilet paper, people need food. If we all panic, nobody has anything, and if nobody has anything, then there’s more panic – it becomes a vicious cycle. Be considerate of others. Take what you need and leave the shop. Let’s act like we live in a community, not just by ourselves.
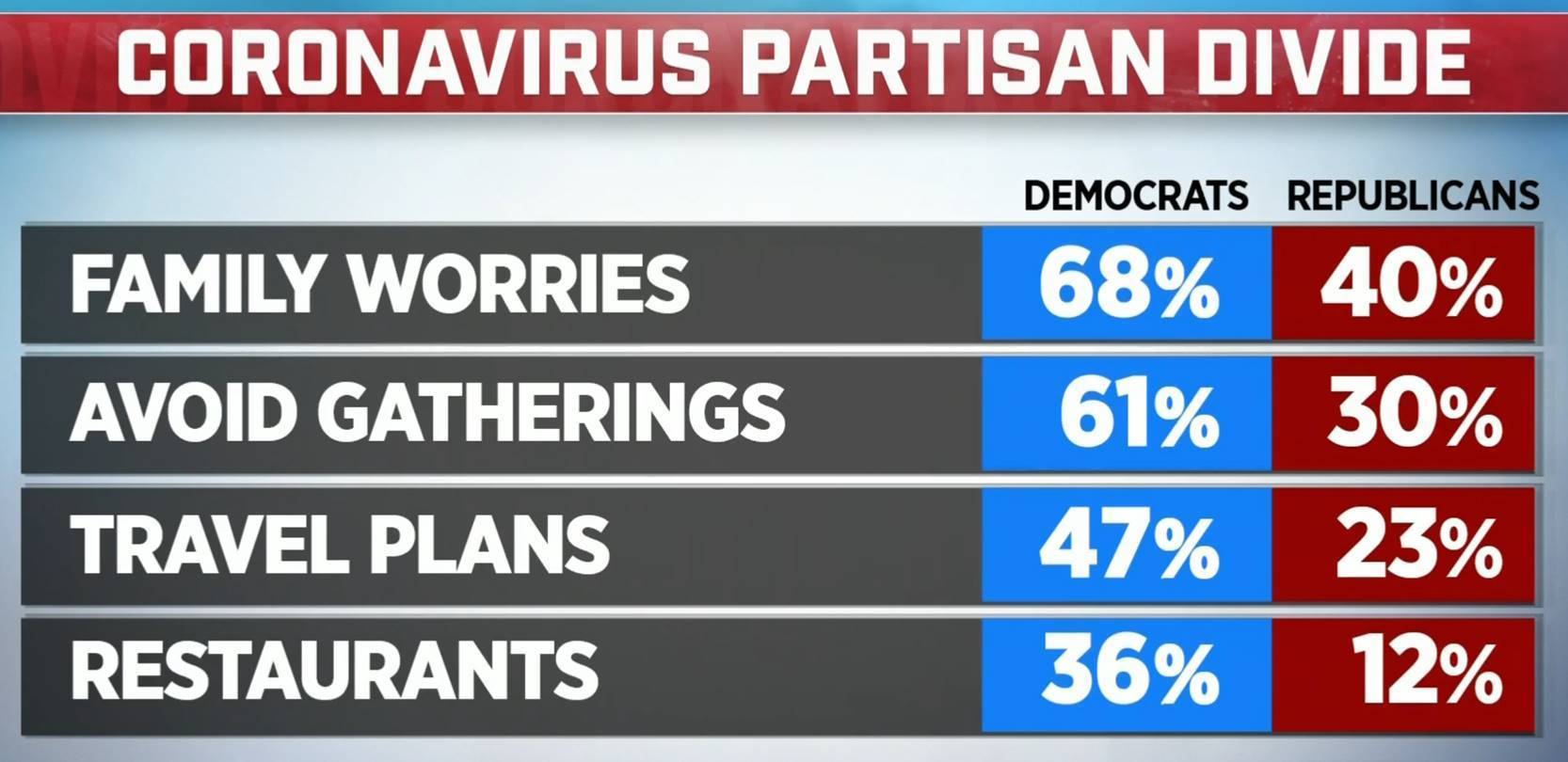
20) This partisan divide on CV cases is super dangerous: Only 30 percent of Republicans are likely to avoid gatherings during coronavirus pandemic (3 min video). Could you imagine if there were such a partisan split among diabetics taking insulin or cancer patients getting chemo???